The legislation authorizing the Title V MCH Block Grant is broad, encompassing a wide array of direct services to individuals and population-based programs that serve everyone in a community. As a “block grant,” states and territories program their MCH investments to meet their specific needs. Through a thorough process that identifies all potential MCH priorities, states and territories conduct surveys and analyze data to determine where they can have the most impact and need the most resources to address MCH problems and challenges. Every year states and territories submit an application to the Maternal and Child Health Bureau (MCHB) of the Health Resources and Services Administration (HRSA) for MCH funding. A formula is used to determine funding allocations based on population size and need.
Over the years, the achievements of Title V-supported projects have been integrated into the ongoing care system for children and families. Landmark projects have produced guidelines for child health supervision from infancy through adolescence; influenced the nature of nutrition care during pregnancy and lactation; recommended standards for prenatal care; identified successful strategies for the prevention of childhood injuries; and developed health safety standards for out-of-home child care facilities.
History of Title V
Title V State Profiles
The Title V Maternal and Child (MCH) Block Grant

Fast Facts
- Title V remains the only Federal program that focuses solely on improving the health of all mothers and children.
- Title V is a partnership with State Maternal and Child Health (MCH) and Children with Special Health Care Needs (CSHCN) programs, reaching across economic lines to support such core public health functions as resource development, capacity and systems building, population-based functions such as public information and education, knowledge development, outreach and program linkage, technical assistance to communities, and provider training.
- Title V makes a special effort to build community capacity to deliver such enabling services as care coordination, transportation, home visiting, and nutrition counseling, which complement and help ensure the success of State Medicaid and SCHIP medical assistance programs.
- Title V funds support programs for children with special health needs to facilitate the development of family-centered, community-based, coordinated systems of care.
- Title V-supported programs provide gap-filling prenatal health services to 2 million women and primary and preventive health care to more than 17 million children, including almost 1 million children with special health needs.

Spotlight! The Adolescent & Young Adult (AYA) Health National Resource Center: How We Support Title V Programs to Advance AYA Health
Anna Corona We're excited to present this blog entry as we approach Mental Health Awareness Month in May. Here at the Adolescent & Young Adult Health National Resource Center (AYAH-NRC), we have a lot to learn from this community of adolescent health champions. We...
Quality Improvement to Support the Transition from Pediatric to Young Adult Health Care
Experiences of the Oregon Children with Medical Complexity CoIIN Team The Collaborative Improvement and Innovation Network (CoIIN) to Advance Care for Children with Medical Complexity (CMC), which is funded through HRSA’s Maternal and Child Health Bureau, is a...
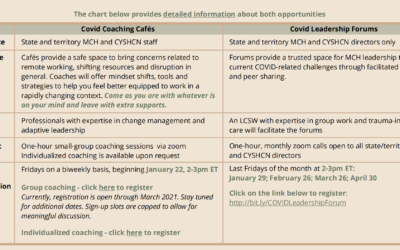
New AMCHP Programs to Support MCH/CYSHCN Staff During the Pandemic
The pressure caused by the COVID-19 pandemic is challenging to early career and seasoned staff alike. AMCHP is pleased to offer two unique programs to support MCH/CYSHCN staff and leadership during the on-going public health emergency: MCH Covid Coaching Cafés are...