How Do We Get Down to Zero?
By Gail Bolan, M.D.
Director, Division of STD Prevention
Centers for Disease Control and Prevention
The data* on syphilis among women and newborns are startling:
- In 2015, women accounted for about one in 10 syphilis cases.
- National data show a 25 percent increase in syphilis among pregnant women from 2012-2014.
- In 2014, nearly one in five women with syphilis was pregnant.
Paralleling the increase in syphilis among women of reproductive age is a sharp increase in the number of babies born with congenital syphilis (CS). In fact, we are witnessing the highest number of CS cases since 2001.
Each case is a needless tragedy and points to missed opportunities for prevention. Almost one-quarter of CS cases are due to a lack of any prenatal care. Although the majority of pregnant women infected with syphilis receive some prenatal care, maternal syphilis is often detected and treated too late to prevent CS. Of women who gave birth to an infant with CS, 42 percent were not tested in time to be treated to prevent CS.
| With nearly 500 cases of CS in 2015 – and preliminary data suggesting these numbers rose in 2016 – the time for action is now. |
The dangers of syphilis infection during pregnancy – and the significant health problems for an infant – cannot be overstated. Historical data indicate that up to 40 percent of pregnancies in women with untreated syphilis will result in miscarriage, stillbirth or infant death. Infants with untreated syphilis may develop severe illness, including deformed bones; severe anemia (low blood count); enlarged liver or spleen; blindness; deafness; or meningitis, which can cause developmental delays and seizures. And yet, congenital syphilis is preventable.
CDC’s Call to Action Outlines Your Role
The Centers for Disease Control and Prevention (CDC) is encouraging public and private sectors, as well as affected communities, to help reduce syphilis through research, outreach and prevention. Last month, we released CDC’s Call to Action: Let’s Work Together to Stem the Tide of Rising Syphilis in the United States. Major efforts are needed to disrupt syphilis. But for our efforts to be effective, we need everyone to pitch in with specific action steps encouraged in the Call to Action.
We are calling on health departments to:
- Partner with health care providers to ensure they receive proper training and education on how to screen, interpret results, diagnose and treat syphilis.
- Also, work together with providers to conduct targeted syphilis screening in various settings.
- Collaborate with state and local STD and Maternal and Child Health programs.
- Prioritize partner services for syphilis cases among pregnant women and women of reproductive age, their sex partners, and men who have sex with women.
- Partner with patient advocacy groups to develop and promote programs directed toward their community’s residents.
- Work to improve CS surveillance by eliminating data gaps.
We are calling on health care providers to:
- Complete a sexual history and risk assessment for all of your patients and provide STD prevention counseling and contraceptive services when indicated.
- Test all pregnant women for syphilis at their first prenatal visit and repeat screening at the beginning of the third trimester and at delivery for those at high risk (including uninsured women, women living in poverty, sex workers and illicit drug users), or who live in communities where syphilis is common among women or where cases of CS are occurring.
- Treat women infected with syphilis immediately with long-acting penicillin G. Also test and treat all sex partners to avoid reinfection.
- Before discharging a mother or infant from the hospital, make sure the mother has been tested for syphilis at least once during pregnancy or at delivery. Manage the infant appropriately if the mother tests positive and has not been adequately treated. And test all women who deliver a stillborn infant for syphilis.
- Report all cases of syphilis by stage and CS to the local or state health department right away. CS cases should be reported within 24 hours.
We are calling on decisionmakers and community leaders to:
- Talk to STD program professionals in your jurisdiction to find out what the local syphilis trends are and what the public health programs are doing to address them.
- Address policy barriers to ensure that policies support pregnant women who seek or obtain prenatal services as well as recommended screening and treatment for syphilis.
- Support the availability of appropriate resources for CS prevention programs.
While the efforts by health care providers, public health departments and decision-makers can make a huge difference, it will not put a full stop to this disease. For these reasons, the Call to Action also outlines steps needed from affected communities, universities, industry and even electronic medical records vendors.
I understand that we are asking a lot from everyone. The CDC is committed to undoing the worsening CS trends with you. We pledge to improve CS surveillance; investigate CS cases to improve services; develop tools and evaluate high-impact prevention services; develop CS prevention guidelines for health care providers and health departments; identify and share best practices; and support health care providers through training, guidelines, tools and resources.
Together we can put syphilis behind us, where it belongs.
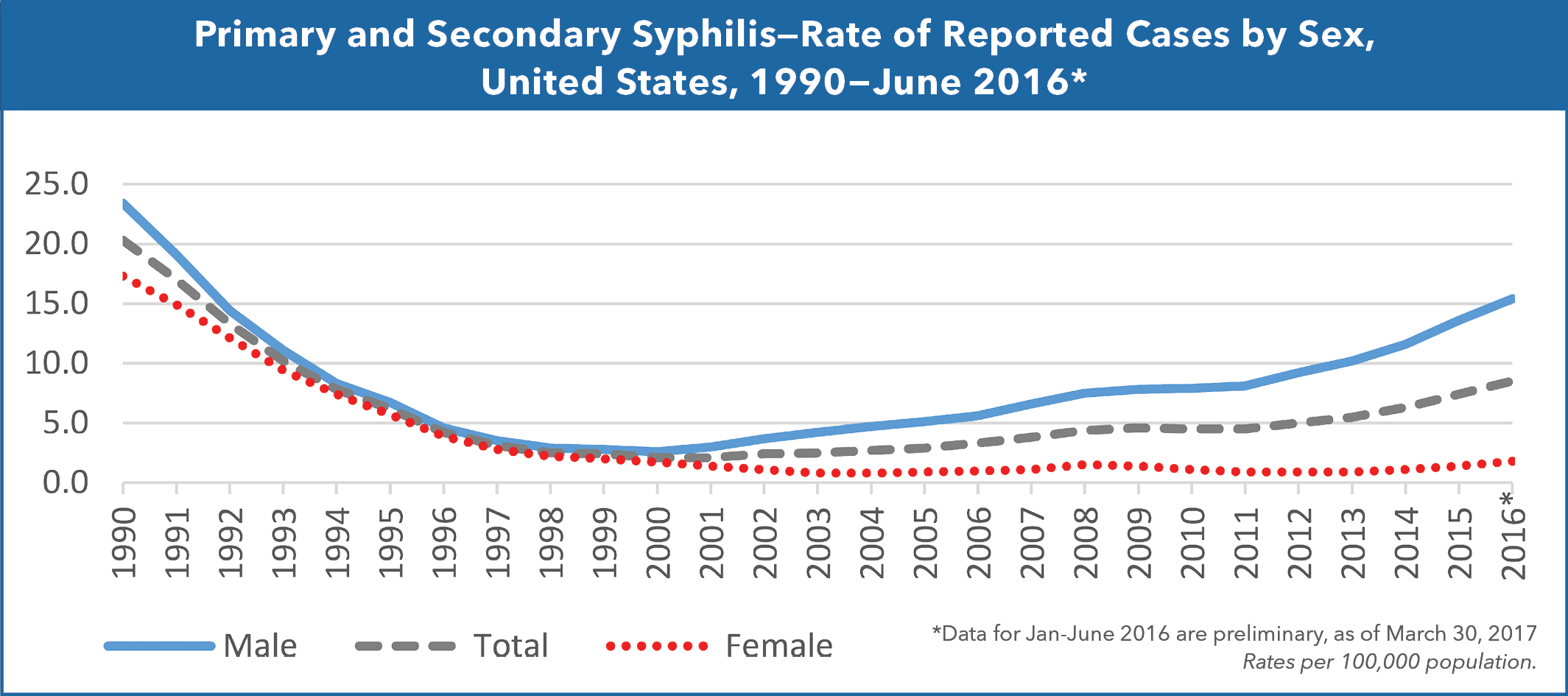
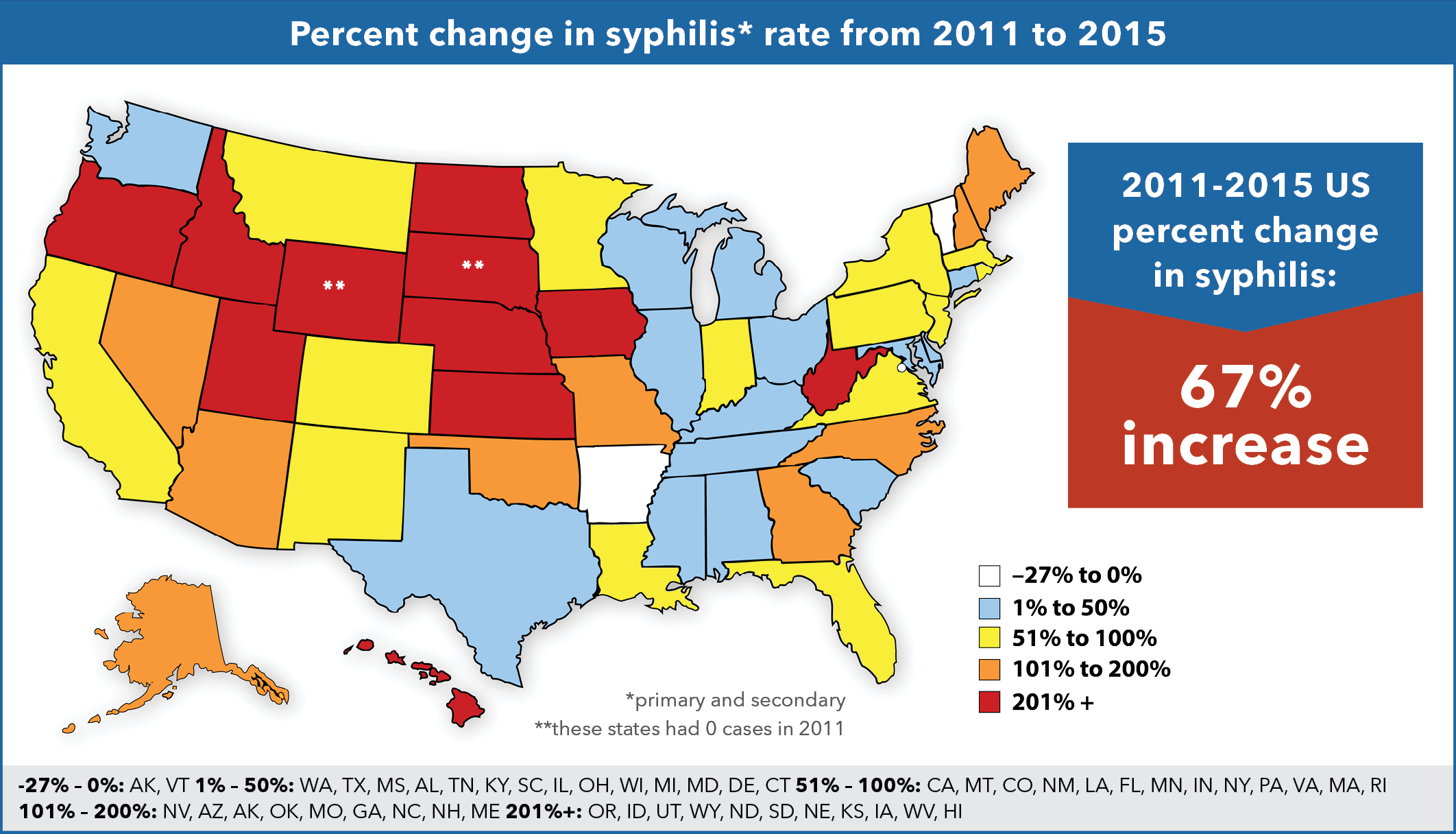
*All data and charts are from the CDC.