Maura Leahy
Program Associate, Child and Adolescent Health
The Association of Maternal & Child Health Programs (AMCHP)
Rose Cutting
Aiming for Acceptance
For children with autism spectrum disorder and other developmental disabilities (ASD/DD), inequities based on race, ethnicity, socioeconomic status, and location of residence can make it exceedingly difficult for them and their families to reach their full potential for health and life in their community. Using data and quality improvement (QI) strategies can identify modifiable, actionable aspects of providing access and coordinated care delivery to advance health equity.
At a recent State Public Health Autism Resource Center (SPHARC) Peer-to-Peer Exchange, Wisconsin’s Health Resources and Services Administration state autism grantee team shared how they were digging into their data and engaging individuals most affected by inequity to ensure that change efforts are locally valued, effective, and sustainable.
The Wisconsin team shared how data can be used to shed light on health disparities, but that the type of data we collect and how we collect it needs to be informed by the needs of the community, or we run the risk of having biased data. Maureen Durkin, PhD shared an example from the Autism and Developmental Disabilities Monitoring (ADDM) Network, citing the prevalence of ASD/DD among 8-year-old children in the U.S. as well as trends in prevalence by sex and race/ethnicity. In 2014, ADDM data estimated the prevalence of ASD among 8-year-old children (per 1,000 children) to be:
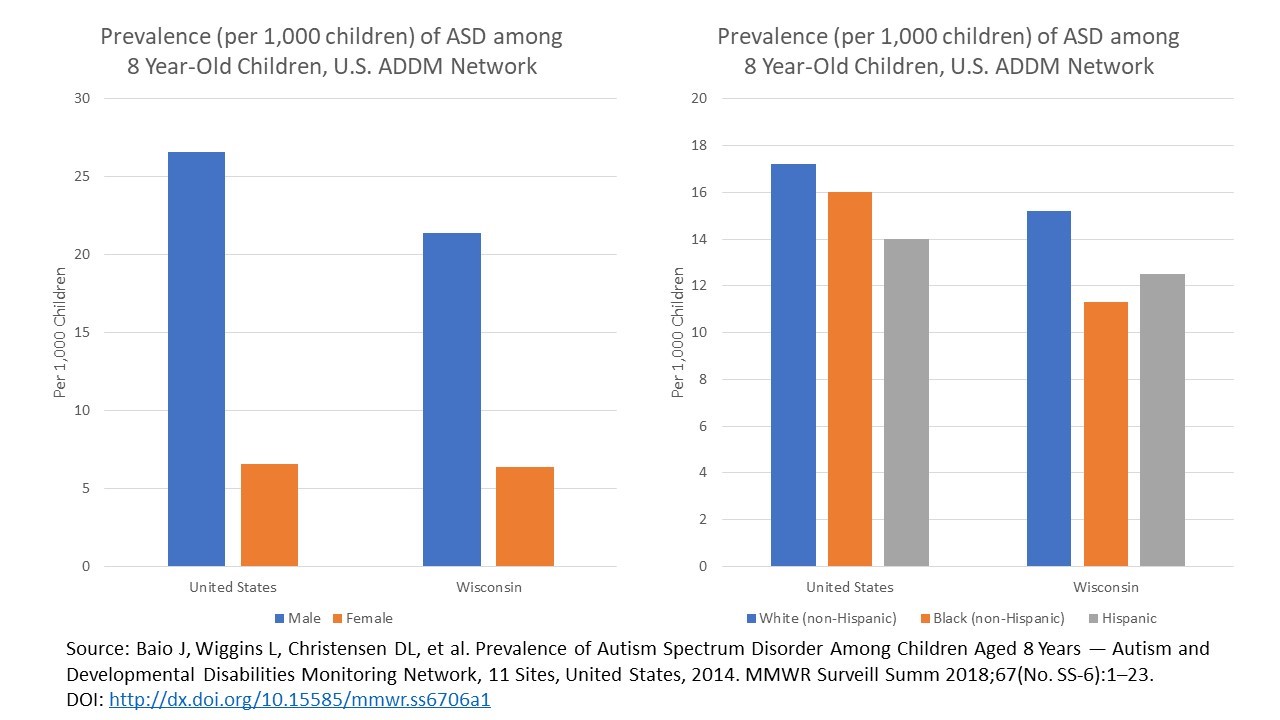
Durkin further engaged participants with the following question:
“Looking at this data, one may conclude that white male boys are more likely to have ASD/DD. But what happens when you add another data variable to the equation? Are there any biases to be considered?”
Durkin then explained how she and other researchers applied a critical lens to the data by considering how a child’s larger environmental context may influence what gets reported in the data. After adding socioeconomic status (SES) to the analysis, looking at both national and state-level data, a curious SES gradient emerged that suggested that children of higher SES had a higher prevalence of ASD/DD. Did this association mean that ASD/DD was more prevalent among white, male children with higher SES?
Durkin and her colleagues took a closer look at the ways in which children were identified with ASD. They posit that the disparity likely lies in unequal access to services and diagnosis for black and Hispanic children, which means their outcomes are missing from the data altogether. As this example demonstrates, without considering the context of the data that we use to make decisions about resource allocation, we risk the perpetuation of inequities in ASD/DD prevalence and by extension contribute to inequities in ASD/DD programs and funding.
Reflections from one Wisconsin Community
To provide real-life context from a community involved with the Wisconsin state autism grantee team, AMCHP staff reached out to Rose Cutting of Aiming for Acceptance, a meeting participant who works in a medically underserved area to support children with ASD and their families. Below, Rose speaks to her efforts to engage stakeholders in defining and addressing equity concerns, and specifically how living in a low-income rural area affects diagnosis of ASD/DD and access to services.
Health equity for my community will not look like health equity for Milwaukee or other cities, nor should it. Health equity is distinct for different communities because we are talking about equity, not equality. Based on my life experience, and from stories gathered from conversations with other families, small business owners, and community members, southwest Wisconsin is eager to build upon its current efforts to become a community in which all members have the opportunity to reach their fullest potential.
One major opportunity is creating universal access to different therapies and resources, such as occupational therapy, that allow the possibility of living one’s best life – therapies and resources that exist only in more populated urban areas. Without this local access, families living in rural areas are forced to drive 40-plus miles, sometimes crossing state lines to Dubuque, Iowa, more than 70 miles to Madison, Wisc., or even 150-plus miles to Milwaukee, Wisc. Focusing strategies to improve local access would have many benefits, including:
- Individuals and families feel supported in the community where they live, work, and play.
- The stress of simply making it to an appointment is reduced, thus opening the opportunity for caregivers to learn more effectively and support others who are in similar situations.
- Families can stay at their farms or small-town businesses, thereby having access to the whole community and its economy benefits.
When there is health equity where I live, the community environment may result in increased positive awareness, acceptance, education, and empowering opportunities that occur naturally in an accessible and sustainable manner. We have an awesome support system, in which members come out in numbers if someone is in need, but there is a lack of education around the needs of individuals with ASD/DD and authority figures to organize what is needed.
Because of reduced local access to therapies and resources negatively impacting those who need services the most, we have children unable to be productive contributors to our communities and eventually being totally dependent on the community to take care of them. But as my grandma used to say, ‘can’t never even tried.‘ Well, we are trying, and in time we will.
—
The topics and discussions at this meeting led to some unanswered questions to explore, and left AMCHP staff reflecting on health equity and the role it plays, or should play, in this work. At AMCHP, we envision a nation that optimizes health for children and youth with special health care needs by supporting comprehensive, coordinated systems of care that engage families and enable all children and youth to live their best life. As such, we invite you to continue this focus on health equity with us and continue the dialogue and discussion of the role of health equity in ASD/DD diagnosis and services and for the MCH population as a whole. For more information and resources, visit the SPHARC homepage or click here to learn what other states are doing around this topic.