Andria Cornell, MSPH
Senior Program Manager, Women’s Health
AMCHP
The inequity by race and ethnicity that characterizes maternal mortality in the United States was a focal point of numerous discussions at AMCHP 2018. A tremendous panel of speakers from the Black Mamas Matter Alliance, University of California at San Francisco, and the Center for Reproductive Rights spoke clearly to Title V programs about their roles in ensuring safe and respectful maternal health care and the incorporation of human rights into policies and programs. Through their session, “Addressing the Maternal Health Disparity Gap Through Advocacy and Community Engagement: A Human Rights and Reproductive Justice Approach,” they provided a language and structure for advancing dialogue. Attendees said the content that resonated with them included re-framing the risk factor from “race” to “racism” and looking critically at how the narrative surrounding a health outcome – including its emergence and response – reflects racism and the unequal valuation of individuals.
The discussion spotlighted a continuing challenge: Maternal and child health (MCH) programs wrestle with identifying policies and programs that address racial and social inequalities. One impediment is that policies and programs that transform community conditions take a long time to show effectiveness. Another impediment is they are often rated lower on a traditional continuum of scientific evidence. One source that MCH programs can turn to for translating data into population-based action is maternal mortality review committees (MMRCs), which craft recommendations from deliberating the causes, critical factors, and preventability of individual maternal deaths.
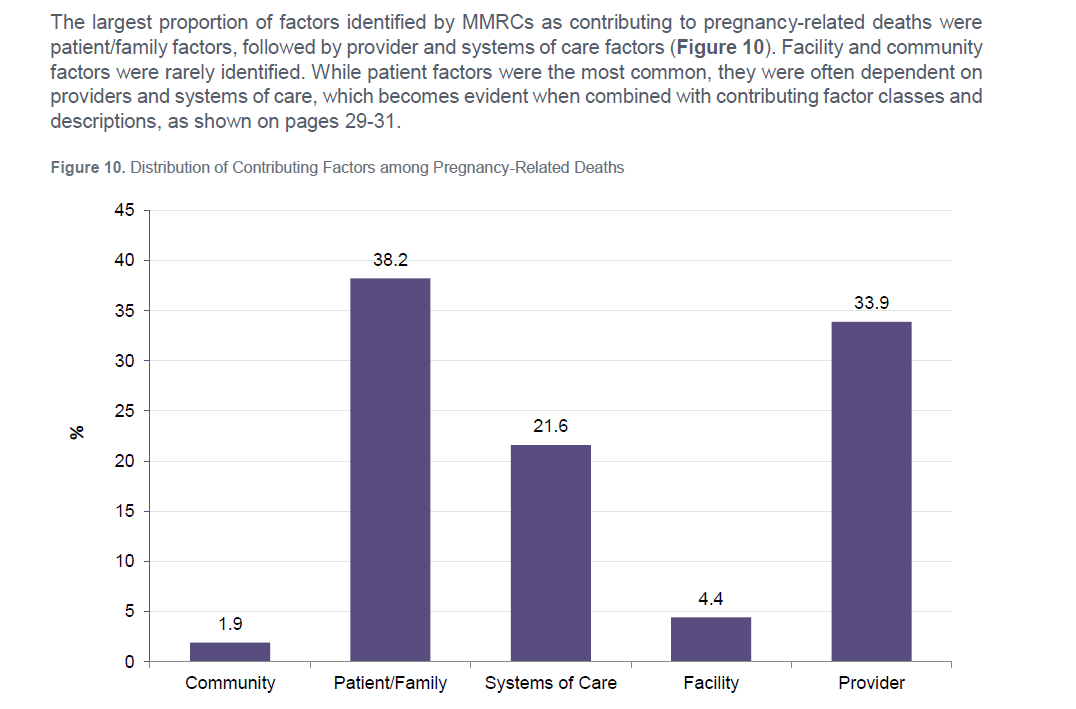
However, making actionable recommendations to advance equity is a challenge for most MMRCs. In a recent report of nine MMRCs’ data analyzed by the Building U.S. Capacity to Review and Prevent Maternal Deaths project, community factors were rarely identified by MMRCs as contributing to pregnancy-related deaths. This does not align with what we know about the socio-ecological model and the causal role of social determinants of health and community conditions. This points to a new frontier for MMRCs and an opportunity to lead their MCH colleagues in a critical assessment of how the way that we collect data matters.
There are a few reasons that MMRCs do not identify community factors as contributing to maternal deaths. One is that a review committee did not have information about the conditions in the community in which the woman lived to be able to evaluate their contribution to her death. There have been some recent advancements to address this gap:
- As part of the Building U.S. Capacity to Review and Prevent Maternal Deaths project, the team at the CDC Division of Reproductive Health and CDC Foundation identified and integrated an equity framework into the Maternal Mortality Review Information Application. Socio-spatial indicators can be used with the geo-coded residential address to characterize the woman’s residential health environment and its difference from other places (e.g., in the state or nationwide). This information can be used to enrich the case review process and data analysis. See page 47 of the nine-committee report for more information.
- The Virginia Pregnancy-Associated Mortality Review embarked on embedding a reproductive justice framework into its case deliberation by including policy and regional issues that could have contributed to the case. MMRCs can reach out to Virginia to learn more and consider how this approach could be applied to their own processes.
- Increasingly, MMRCs are exploring the incorporation of informant interviews with family, friends, and community members connected to cases. Most data sources provide only surface-level information, which says little about the context of a woman’s life. While informant interviewing is a resource-intensive process that might not be feasible for every death in some states, the process communicates the value of, and a willingness to listen to, the families and communities affected by the death.
A second reason MMRCs might not identify community factors as contributing to maternal deaths may be misperception of, discomfort with, or lack of experience discussing the role community conditions play in maternal health and their modifiability. Even if MMRCs have access to data or information about those conditions, deliberating their causal role in the maternal death can be challenging.
To overcome this barrier, some MMRCs are reexamining their committee membership. MMRCs have existed in the United States for more than a century. Originally, these committees were composed primarily of obstetricians. They have since expanded their membership to include a vast array of professionals and partners engaging with and serving women during pregnancy and the year postpartum.
As demonstrated through the discussion following the AMCHP conference session, “Leveraging Polices and Partners to Establish and Sustain Maternal Mortality Review,” many MMRCs want to further expand their membership to prioritize the engagement of women and community champions. These MMRCs recognize that the quality of a case review, deliberations about individual deaths, and ultimately the recommendations that are crafted directly align with who is around the table. This will be an area of focus for AMCHP in 2018.
Here are some places review committees can start:
- Look at the authorizing legislation for the MMRC. In some states, the legislation outlines the process through which committee members can be identified and appointed. For states interested in passing standalone legislation detailing key authorities and protections for the MMRC, stakeholders can specify community organization or survivors of a severe maternal morbidity to serve on the MMRC. In the Authorities and Protections checklist, Review to Action provides an example of legislative language from Texas.
- Reconsider recruitment practices for new members. When filling vacancies, MMRCs should not rely on who is already known to the group. Ask around, be intentional, and reach out to champions from the communities the MMRC serves. For example, MMRCs can connect with states that have Healthy Start sites or other community organizations serving on their MMRCs to learn about their successes. Interested in where to start? Contact the National Healthy Start Association or the Florida Pregnancy-Associated Mortality Review, which has an extended and fruitful partnership with REACH UP, Inc., in the implementation of its review.
- Listen. Each member brings unique expertise and perspective to the case deliberation. Respect and value the voices of the women and community champions engaged by the MMRC. Recommendations for the facilitative group process are detailed in Appendix E of the Committee Facilitation Guide.
- Build capacity. Invest in training community members about the surveillance process and the systems it supports as a part of onboarding to the MMRC. MMRCs may wish to be explicit about the group norms and the value placed on community voices as a part of their documented policies and procedures.
- Engage women in developing MMRC communication products. As Dr. Joia Crear-Perry has cautioned, how data are sent out matters because policies are consequentially shaped by that data collection and dissemination. MMRCs can create their reports and briefs in partnership with community stakeholders to ensure recommendations are feasible, align with community values, and are positioned to be implemented in partnership with communities.
AMCHP is committed to collaborating with its members and partners in identifying and communicating practices across the evidence spectrum to advance maternal health equity and center women’s voices in crafting the path forward. Know of a practice or activity not highlighted here, or want to brainstorm with us? Contact mmr@amchp.org.
Building U.S. Capacity to Review and Prevent Maternal Deaths